.png)

Did someone forward you this email? Sign up here.
Dear readers,
For the last few years, one of my favorite parts of Tangle has been hiring young writers and giving them an opportunity to work with us. Over the years we’ve had a number of “interns” (nobody really does intern work here) who have made major contributions to our newsletter, gone on to work for awesome publications, or left and returned years later to work for us.
Last year, our managing editor Ari Weitzman decided to formalize this experience with a six-month fellowship program. We got dozens of applications, and ended up hiring Hunter Casperson — a sharp writer and recent journalism master’s graduate from California. Hunter immediately earned a reputation for thoughtful edits, speaking her mind, and stepping up to do whatever was asked of her.
This month, her six months at Tangle are coming to a close. In the past, it’s been simply tradition that we’ve let Tangle interns write a capstone piece — this year, with the process formalized, we baked it into the initial schedule of working with Hunter. The prompt is simple: You can pick any topic you want to cover, and we’ll work on a well researched, long-form piece with you that we’ll publish as a Friday edition. Today, we are sharing Hunter’s capstone piece.
It is, in my estimation, perfectly Tangle. It covers a controversial topic. It’s personal. It is deeply researched. It is thoughtfully written. And most importantly, it offers fair treatment of a complicated issue. I hope you enjoy it, and I want to thank Hunter for all her contributions to Tangle — I’m excited to see what she does next!
Best,
Isaac Saul
Introduction.
I learned I was autistic when I was swimming at an apartment pool with my sister last summer.
We had gone swimming to escape the thick Texas heat, and I started telling her about a fight I had with my roommate, a fight that I didn’t really understand. I said, “It’s so frustrating. It’s like people will tell me what I did wrong and as soon as they tell me it’s so obvious and I feel horrible, but if they don’t tell me directly I’d never figure it out.” After a thoughtful pause, my sister — who was studying psychiatry — deadpanned me with, “Hunter, have you ever considered that you might be autistic?”
For some reason, in that moment, the realization hit me like a meteorite to the face. It made so much sense, and at the same time… didn’t? I would have known if I was autistic, right? I’ve always been “the social kid,” so I can’t be autistic — that doesn’t make any sense.
Turns out it did make sense. Fast forward three months after seeking a diagnosis and doing a lot of research, I had learned that what I really had was unofficially referred to as AuDHD, a combination of autism and Attention Deficit Hyperactivity Disorder (ADHD) that can look very different from what people typically associate with autism. I learned that people with AuDHD typically:
- Blurt out shocking, inappropriate things that often get laughed off
- Seek social interaction, but often find themselves feeling dissociative and disconnected from their social environment
- Crave stimulation and change, but simultaneously feel most comfortable when things are predictable and constant
Check, check, and check.
I also found that the more I learned about my AuDHD, the more I learned how flawed our society’s general understanding of neurodivergence is.
ADHD is a prime example. Despite ADHD having been researched since the start of the 20th century, systematic research on ADHD in women did not occur until 1979. Consequently, our entire understanding of ADHD was built off of its manifestation in boys and men, and as it happens, it typically looks really, really different in women. For example, girls are socially conditioned to be less hyperactive than boys, which is a key symptom used to diagnose ADHD. Consequently, many girls and women went undiagnosed for decades, but as new research came out and our understanding broadened, the number of diagnoses skyrocketed. However, it is noteworthy that we are still dealing with the consequences of 80 years of delayed research today — in clinical studies with children, the male to female diagnosis ratio is 4:1, and in community or population studies, the ratio is approximately 2:1.
Autism, so far, seems to have followed a similar path in the sense that there is very limited research about it, and therefore the general public’s understanding of autism is very skewed. This has led to very tangible, real impacts.
A few weeks ago, I was reading an opinion piece in The New York Times called “Should Human Life Be Optimized?” by Anna Louie Sussman. The piece discussed Preimplantation Genetic Testing (PGT) in In Vitro Fertilization (IVF).
In the article, Sussman interviews Noor Siddiqui, the founder of the genetic screening company Orchid. Siddiqui stated that she envisions a future where “sex is for fun, and embryo screening is for babies,” stating, “It’s going to become insane not to screen for these things.”
Then, I read the line that made my stomach drop: “‘These things’ presumably refers to conditions like obesity and autism, both of which Orchid says it can screen for, ” Sussman wrote.
My first thought was, Is this actually happening? The answer — of course — is that it’s complicated.
What is Preimplantation Genetic Testing (PGT)?
In Vitro Fertilization (IVF) is a method of laboratory-assisted reproduction in which an egg is fertilized with sperm in a laboratory dish before the resultant embryo is implanted into a woman’s uterus. People use IVF for a variety of reasons, including overcoming infertility, preserving fertility, having a child as a same-sex couple or as a single individual. In many cases, those using IVF will choose to genetically test potential embryos. Multiple embryos are created during the IVF process, but typically only one is implanted, allowing individuals and couples to choose which embryo they want based on the results of the testing. The unchosen embryos are either frozen, donated, or discarded as medical waste.
There are three main types of Preimplantation Genetic Testing (PGT): PGT-Aneuploidy (A), PGT-Monogenic (M), and PGT-Polygenic (P). PGT-A evaluates an embryo’s chromosomes, looking for either missing chromosomes or additional chromosome material, either of which may indicate a higher risk of a miscarriage, implant failure, or impact the health of a future child. PGT-A can detect conditions like Down syndrome and Turner syndrome, and can also be used to identify the sex of an embryo based on the shape of the sex chromosomes. While PGT-A can be performed for any patient, it is typically recommended for female donors over the age of 35.
PGT-M is typically used when a genetic condition runs in a family. PGT-M detects single-gene mutations, like the BRCA gene that indicates a higher risk of breast cancer, to determine whether the embryo carries the mutation, allowing couples to choose whether or not to implant an embryo.
The third type, PGT-P, targets the entire genome, allowing embryonic testing to assess the risk of an embryo developing certain polygenic conditions, such as autism. These conditions are more complex than monogenetic disorders as they are influenced by multiple genes and environmental factors. I spoke with UCLA genetics researcher Daniel Benjamin, who explained the difference of PGT-P: “For most traits, including many diseases like diabetes and cardiovascular disease, there's no single gene that causes the disease. There's thousands of genes spread across the whole genome that contribute each a tiny little bit. PGT-P measures thousands of genes and adds up what's known about their effects to probabilistically estimate a likelihood of getting that trait.”
Embryonic testing is not required for IVF and is considered an optional procedure. There is a wide range of pricing for embryonic testing depending on factors such as number of embryos, method of testing, and lab selection.
PGT policy and use.
Across the globe, cultural, moral, and ethical divides have created major disparities in how genetic testing is regulated. On the lenient end of the spectrum, with no legislative regulation, are the U.S. and Mexico. Although professional organizations like the American Society for Reproductive Medicine have issued opinions on best practices, embryonic testing is widely accepted in the U.S., and its use has become largely commercialized for both medical and nonmedical reasons. For example, there are currently options available like Nucleus Embryo, a “genetic optimization software” that provides a full genetic profile on each embryo. The details are categorized into groups: appearance, body, cancers, female/male health, food and diet, heart, mind, and other. Traits included in these categories are: eye color, height, severe acne, left-handedness, BMI, ADHD, IQ, asthma, seasonal allergies, and many more. You can explore the full demo and see the full profiles here.
On the other end of the spectrum are countries like Germany, Switzerland and Austria, which have far more stringent legislation prohibiting various uses of PGT. In Austria, for example, cases deemed “appropriate use” are classified as instances in which a child would either become so ill during pregnancy or after birth that it would suffer brain damage, experience severe pain that could not be effectively treated in the long term, or could only be kept alive through the constant use of modern medical technology, nursing aids, or other medical aids that would severely impair their quality of life.
Countries such as Brazil, Israel, and Japan land somewhere in the middle. Despite not having legislative restrictions, cultural and societal differences have made the widespread use of embryonic testing far less common in these examples than in the U.S. Other countries like the United Kingdom and South Korea have regulatory legislation, but still support the use of PGT for various, preapproved medical conditions.
Below is a chart from a 2020 study surveying 19 countries and their policies on PGT.
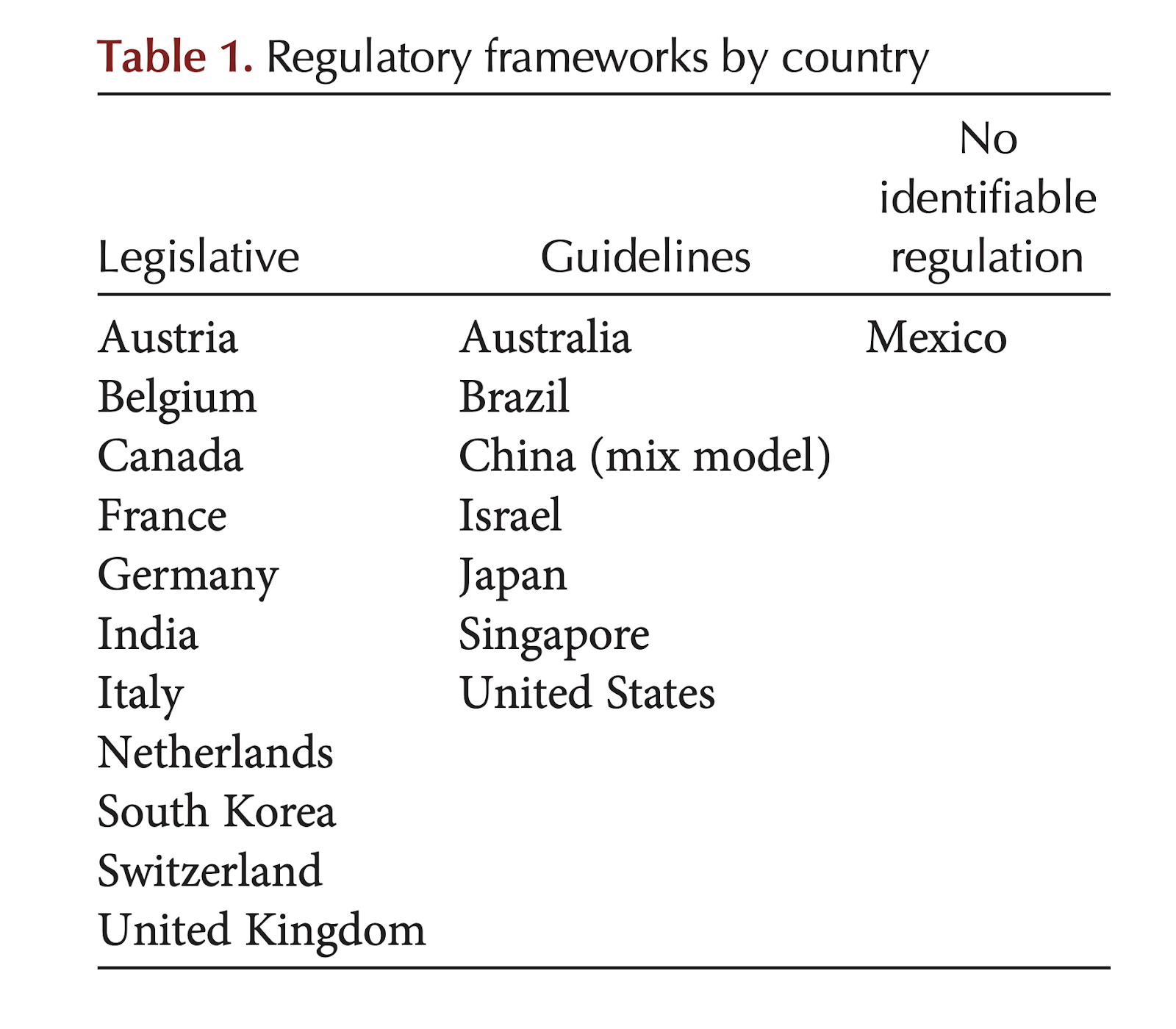 Perspectives in Medicine, 2020 | https://perspectivesinmedicine.cshlp.org/content/10/5/a036681.full.pdf+html
Perspectives in Medicine, 2020 | https://perspectivesinmedicine.cshlp.org/content/10/5/a036681.full.pdf+htmlArguments in favor of embryonic testing.
Broadly, proponents of PGT-A, which tests for sex and chromosomes, highlight the significantly increased rates of successful implantations when using PGT-A as opposed to not. Since many patients accessing IVF are battling infertility, upping the odds of successful implantation and decreasing the odds of a miscarriage can provide huge incentives for testing. “A significant benefit of PGS/PGT-A is the reduced level of uncertainty patients may experience before and after the embryo transfer,” Pacific Fertility Center Los Angeles wrote. “PGS provides you with an ensured healthy embryo, a lower risk of pregnancy loss, and less emotional stress, especially for patients who’ve experienced the saddening loss of miscarriage before.”


